2019: Latest Information
Dramatic increases in dental fluorosis point to widespread fluoride overexposure with risk of neurotoxicity
March 15, 2019 – Researchers report a huge increase in dental fluorosis in the USA in a paper just published in the Journal of Dental Research – Clinical & Translational Research.
Dental fluorosis is a tooth enamel defect caused by excessive fluoride intake during childhood. It appears as white spots or lines in milder cases and pitted and stained enamel in more severe cases. Analysis of the most recently available government data (NHANES 2011-2012 survey) found that 65% of American children now have some degree of dental fluorosis.
The survey found the objectionable degrees of dental fluorosis, termed “moderate” and “severe”, in 30.4% of children age 12-15. This was an 8-fold increase from the previous national survey in 1999-2004 that found 3.7% affected.
Paul Connett PhD, director of Fluoride Action Network, noted: “This is compelling evidence that fluoride exposure, linked to lowered IQ in children, has skyrocketed. Fluorosis is a permanent marker of excessive early life exposure to fluoride. The US Public Health Service (PHS) has promoted fluoridation since the 1950s, but now must recognize fluoride exposure is out of control. The emerging evidence of harm to developing brains can no longer be dismissed.”
According to lead author, Chris Neurath: “These extremely high rates are unprecedented and far beyond what were considered acceptable when water fluoridation was started 75 years ago.”
“Although we were not able to determine what specific sources of fluoride caused these large increases in fluorosis, likely contributors include increases in water fluoridation, especially when used for mixing infant formula, and swallowed fluoride toothpaste.”
“The PHS in 2015 recommended a reduction in the level of fluoride added to drinking water. This was a response to the increase in fluorosis between 1986-1987 and 1999-2004. The much larger increase in the 2011-2012 survey was apparently not considered. The PHS’s reduction may be insufficient to reduce fluorosis to dentally acceptable levels and ignores the serious neurotoxic effects that may be occurring.”
Neurath also noted: “The rear teeth were usually the most affected and it was their scores that determined the person-level scores. When we only considered the front teeth the ‘moderate’ & ‘severe’ rate was 10% instead of 30%. Many fluoridating countries only consider front teeth in their surveys (Canada, Australia, New Zealand) thereby underestimating true rates of fluorosis.”
See
• the full Paper
• the Appendices for more data
• the Press release
• the Abstract
How to cite the paper:
Neurath C, Limeback H, Osmunson B, Connett M, Kanter V, Wells CR. 2019. Dental Fluorosis Trends in US Oral Health Surveys: 1986 to 2012. JDR Clinical & Translational Research. https://doi.org/10.1177/2380084419830957
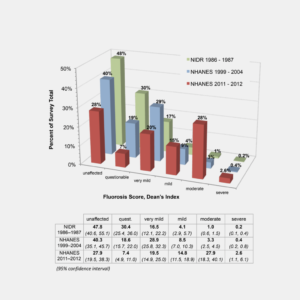
The following two graphics are from the paper.
Figure 1. Dean’s Index score frequency distribution for children ages 12-15 years, comparing changes across the three national surveys in the USA.
 _________________________________________________________
_________________________________________________________
Examples of four degrees of dental fluorosis using Dean’s Index:

A little background on Dental Fluorosis and how we got here
By Daniel Grossman, The Progressive, December 1990
… An investigation of the health effects of fluoride, including two Freedom of Information Act requests that pried loose more than 10,000 pages of documentation, shows that a Government regulation intended to prevent fluorosis was derailed by a decades-old controversy between two agencies over a legally unrelated Government policy.
Officials at the Public Health Service, the Federal Government’s all-purpose health agency, stopped the Environmental Protection Agency from issuing a standard to prevent dental fluorosis because they feared the rule would disrupt their own plans to protect dental health. As a result, what might have been an open public debate became an obscure internecine battle between two bureaucracies, each with its own idea of what makes good public policy. Though dental fluorosis is hardly a life-threatening ailment, this story demonstrates how a powerful agency, intent upon enforcing its own view of the public good, can suppress anyone who gets in its way…
Public Health Service memo never shared with the African American community or with the medical community:
A January 10, 1962 internal memorandum, from a top PHS official, F.J. Maier, in connection with the first fluoridation trial, revealed that, “negroes in Grand Rapids had twice as much [dental] fluorosis than others.” Based on this, Maier asked, “In a community with a larger number of negroes (say in Dekalb County, Georgia) would this tend to change our optimum fluoride levels?”(Maier, 1962).
Important Papers on Dental Fluorosis in the U.S.
• 1977. Drinking Water and Health. Volume 1. National Research Council of the National Academies.
• 1982. Ad Hoc Committee Report on Dental Fluorosis. Public Health Service (PHS), National Institute of Dental Research (NIDR), and Indian Health Service.
• 1985. EPA Administrators decided in 1985 to increase the allowable level of fluoride to 4 ppm, a level that the Agency admitted would produce disfiguring dental fluorosis in 40% of children. On the day the EPA announced its decision, a scientist who worked on the standard circulated a mock press release among staff employees which stated:
“Up to now EPA, under the Safe Drinking Water Act, has regulated fluoride in order to prevent children from having teeth which looked like they had been chewing brown shoe polish and rocks. The old standard . . . generally kept fluoride levels below 2.4mg/L. EPA in response to new studies, which only confirmed the old studies, and some flat out political preasure, has decided to raise the standard to 4 mg/L. This increase will allow 40% of all children to have teeth gross enough to gag a maggot. EPA selected this level based upon a cost effectiveness study which showed that it is cheaper for people to keep their mouths shut then to remove the fluoride.”
• 1985. Perspectives in Disease Prevention and Health Promotion Dental Caries and Community Water Fluoridation Trends — United States. Morbidity and Mortality Weekly Report (MMWR) February 15 / 34(6);77-80,85
• 1991. Review of Fluoride: Benefits and Risks. Department of Health & Human Services, Public Health Service.
• 1993. Health Effects of Ingested Fluoride. National Research Council of the National Academies.
• 2001: CDC: Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States. Adair et al. Morbidity and Mortality Weekly Report (MMWR) August 17/ 50(RR14);1-42.
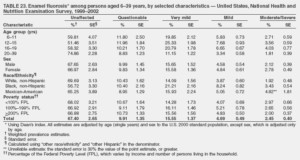
• 2005. CDC: Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism, and Enamel Fluorosis — United States, 1988–1994 and 1999–2002. Beltrán-Aguilar et al. Morbidity and Mortality Weekly Report (MMWR) August 26 / 54(03);1-44 – included this Table
• 2007. Beltram & Barker: Prevalence of Enamel Fluorosis Among 12-19 Year-Olds, U.S., 1999-2004.
• 2011. EPA and HHS Announce New Scientific Assessments and Actions on Fluoride. Press Release. January 7.
• 2011. New Fluoride Risk Assessment and Relative Source Contribution Documents. EPA Press Release. January.
• 2015. Public Health Service Recommendation for Fluoride Concentration in Drinking Water for Prevention of Dental Caries. Federal Register, May 1. (also in pdf)
• 2015. Overview: Infant Formula and Fluorosis. From CDC website. July.
• 2015. Water Fluoridation and Environmental Justice. A report by the Fluoride Action Network and submitted to the Environmental Justice Interagency Working Group. September 25.
• 2016. Federal Register Notice which states, “The following major examination or laboratory items, that had been included in the 2015–2016 NHANES, were cycled out for NHANES 2017–2018: … dental fluorosis assessment, dental fluorosis imaging (DFI), plasma, urine and water fluoride.” November 7.
• 2018. CDC: Public Comments Due Oct 11 on Range for Fluoride Concentration in Fluoridation Schemes. Federal Register, Notice, October 8.
• 2019. CDC: Use of Toothpaste and Toothbrushing Patterns Among Children and Adolescents — United States, 2013–2016. Thornton-Evans et al. Morbidity and Mortality Weekly Report (MMWR) February 1, / 68(4);87–90
More Information
• Dental Fluorosis in the U.S. 1950-2004
• Over 260 published papers on dental fluorosis
• Racial Disparities in Dental Fluorosis
• Dental Fluorosis: The “Cosmetic” Factor
• Severe Dental Fluorosis: Perception and Psychological Impact
• “Mild” Dental Fluorosis: Perceptions & Psychological Impact
• Moderate/Severe Dental Fluorosis
• Dental Fluorosis Is a “Hypo-mineralization” of Enamel
• Mechanisms by Which Fluoride Causes Dental Fluorosis Remain Unknown
• Diagnostic Criteria for Dental Fluorosis: The Thylstrup-Fejerskov (TF) Index
• Diagnostic Criteria for Dental Fluorosis: The TSIF (“Total Surface Index of Fluorosis”)
• Dental Fluorosis Impacts Dentin in Addition to Enamel
• Community Fluorosis Index (CFI)
• Effects of Water Fluoridation on Teeth: Dental Fluorosis vs. Tooth Decay
-
-
The Absurdities of Water Fluoridation
[caption id="attachment_10205" align="alignleft" width="190"] Paul Connett, PhD[/caption] Water fluoridation is a peculiarly American phenomenon. It started at a time when Asbestos lined our pipes, lead was added to gasoline, PCBs filled our transformers and DDT was deemed so "safe and effective" that officials felt no qualms spraying kids in school classrooms
-
Why I am now officially opposed to adding fluoride to drinking water
https://www.youtube.com/watch?v=iF-hKlIgCuM April, 2000 To whom it may concern: Since April of 1999, I have publicly decried the addition of fluoride, especially hydrofluosilicic acid, to drinking water for the purpose of preventing tooth decay. The following summarize my reasons. New evidence for lack of effectiveness of fluoridation in modern times. [caption id="attachment_10211" align="alignleft" width="150"] Dr. Hardy
-
50 Reasons to Oppose Fluoridation
Introduction [caption id="attachment_11821" align="alignleft" width="200"] Dr. Paul Connett[/caption] In Europe, only Ireland (73%), Poland (1%), Serbia (3%), Spain (11%), and the U.K. (11%) fluoridate any of their water. Most developed countries, including Japan and 97% of the western European population, do not consume fluoridated water. In the U.S., about 70% of public water supplies are
Related Articles:
-
-
-
Fluoride & IQ: 76 Studies
Note: See the Updated list of fluoride IQ studies at https://fluoridealert.org/researchers/fluoride-iq-studies/the-fluoride-iq-studies/ • As of July 18, 2022, a total of 85 human studies have investigated the relationship between fluoride and human intelligence. • Of these investigations, 76 studies have reported that elevated fluoride exposure is associated with reduced IQ in humans. • The studies
-
Fluoride's Effect on Fetal Brain
The human placenta does not prevent the passage of fluoride from a pregnant mother's bloodstream to the fetus. As a result, a fetus can be harmed by fluoride ingested pregnancy. Based on research from China, the fetal brain is one of the organs susceptible to fluoride poisoning. As highlighted by the excerpts
-
Fluoride: Developmental Neurotoxicity.
Developmental Neurotoxicity There has been a tremendous amount of research done on the association of exposure to fluoride with developmental neurotoxicity. There are over 60 studies reporting reduced IQ in children and several on the impaired learning/memory in animals. And there are studies which link fluoride to Attention Deficit Hyperactivity Disorder. Teaching
Related Studies:
-
-
-
Email Exchange with FDA re: Fluoride Supplements
Email exchange regarding FDA's reasons for not approving fluoride supplements.
-
Harvard's Statement on Chester Douglass/Scientific Misconduct
Statement Concerning the Outcome of the Review into Allegations of Research Misconduct Involving Fluoride Research BOSTON-August 15, 2006-The Harvard Medical School and School of Dental Medicine (HSDM) review of Chester Douglass, DMD, PhD, professor of oral health policy and epidemiology at HSDM, has concluded that Douglass did not intentionally omit, misrepresent,
-
The 'Altered Recommendations' of the 1983 Surgeon General's Panel
"We believe that EPA staff and managers should be called to testify, along with members of the 1983 Surgeon Generals panel and officials of the Department of Human Services, to explain how the original recommendations of the Surgeon Generals panel were altered to allow EPA to set otherwise unjustifiable drinking water standards for fluoride."
Related Miscellaneous Content:
-


